The Achilles Tendon is one of the largest and strongest tendons in the body. It connects the back of the heel bone (Calcaneus) to the calf muscle (Gastrocnemius and Soleus). This tendon allows running/jumping/walking/lifting to occur normally where the foot is actively plantarflexed. Normally this tendon allows one to go up on the front part of the foot. Without this tendon, you are walking on flat foot that does not actively propel very well.
Generally an Achilles rupture is from a traumatic event. Either sports related, work related, or just normal daily activity. Often doctors will hear a patient comment, "it felt like some one kicked me in the back of the leg. I went to get up and could not use my foot!" Or you may feel like you had a loud "pop" in the back of the leg. The test for an Achilles Tendon rupture involves squeezing the calf muscle and looking for the foot flexing with this motion. If the tendon is intact, this will occur easilly. If it is ruptured, no motion occurs. Occasionally one needs to compare the affected leg to the healthy one. An obvious defect is often seen or felt. In questionable cases, or cases which require additional surgical planning, an MRI may be indicated.

If there is an obvious 1cm gap or greater, surgery is generally recommended. If the gap is able to be brought together with the foot flexed plantarly, a cast may suffice. Cast immobilization would generally be indicated in someone who was mostly sedentary or who was bed bound. For individuals who are fairly active, and who are appropriate surgical candidates, a surgical repair is indicated in almost every case. The risk of re-rupture is higher if you do not have a surgical repair, and you will need to be immobilized for 6-8, and will not be able to put any weight on your foot.
With surgery, passive motion can be started at 1-2 weeks after repair. This is assuming you are healing ideally. Stitches can generally come out at about 2 weeks and you can return to showering. at that time. At 3 weeks after surgical repair, the tendon is at about 50% strength or greater. It could be argued that with surgical repair, the tendon is much stronger than this due to the strength of the sutures themselves. Surgery should be considered carefully, as there are many risks with Achilles Tendon Surgery. But....if you are a person who is fairly active, a surgical repair would usually be recommended.
What are common complications?
In the healthy patient, a full recovery can usually be expected with the appropriate surgical repair. Stiffness and limited range of motion should be expected for several months at least. The surgical repair can be felt through the skin at times. In this location, there is not as good of blood flow and skin healing issues are more likely than many other areas of the body. Again, the most likely people to have post surgical issues are smokers, diabetics, immunocompromised, or the elderly. Infections can occur as with any surgery - they are more difficult to fight in this area because of the decreased blood supply here. Adhesions can occur between the tendon and skin at times as well and the foot will not move as well.
My surgical technique:
An incision is made over the tendon and the paratenon is identified and preserved. This is a thin layer over the tendon similar to a tendon sheath that allows the tendon to glide smoothly beneath the skin. It is important to repair this layer cautiously so that the tendon will function optimally. Once the tendon rupture is identified, the ends are freshened up a bit and then re-approximated if possible.

Traditional Krackow Achilles Repair

Modified Krackow "Giftbox" Achilles Repair
(Suture knots tied away from the gap, dramatically
improving strength with less skin irritation)
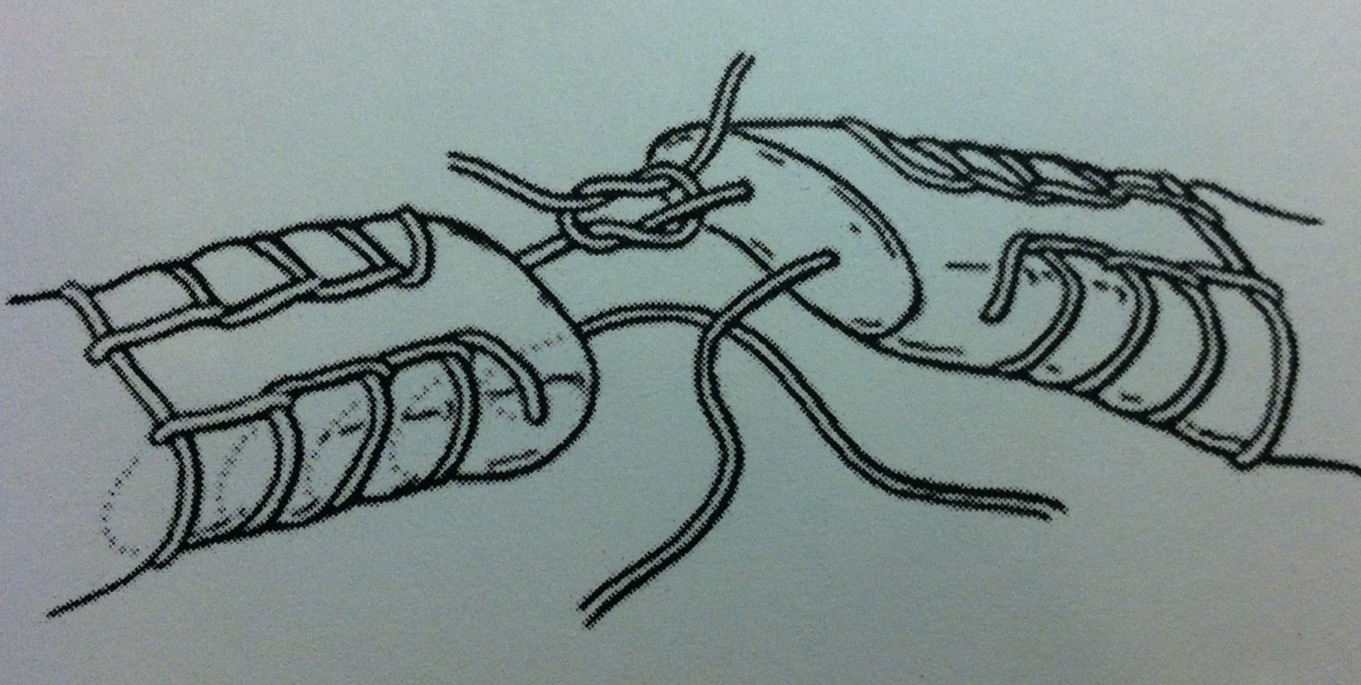
Additionally, the repair is augmented by an epitendinous cross stitch weave (2) which makes it even stronger and makes the tendon smoother. The tendon is able to withstand loads sooner and glides much better by utilizing this specific technique. This has been shown to increase force to failure by 65%. See the drawing and clinical photo below. I have been using this technique for several years now and have been seeing great results. Increased strength of the repair which potentially allows patients to return to activity faster with less down time.

Epitendinous Cross Stitch Weave
1. Labib,S.A. et al. The "Giftbox" Repair of the Achilles Tendon: A Modification of the Krackow Technique. Foot and Ankle International. 2009.
2. Lee, S.J. et al. Optimizing Achilles Tendon Repair: Effect of Epitendinous Suture Augmentation on the Strength of Achilles Tendon Repairs. Foot and Ankle International. 2008.